I first noticed the Abominable Lymph Node (ALN) in February 2005. I was laying on the sofa reading a nonfiction book, 50 Acres and a Poodle, about a woman who says goodbye to city life and moves to a Green Acres-type place. Her boyfriend develops a strange pain in his abdomen, which turns out to be a tumor on the intestine.
The ALN was then only noticeable when I lay flat on my back; there was just a slight sensation of pressure near my left hip, nothing painful. If I lay on my side, or stood up, or sat in
 a chair, I did not notice it. Still, it was a new sensation, not unlike the new sensation the boyfriend in the book had begun to notice. And it definitely wasn’t normal.
a chair, I did not notice it. Still, it was a new sensation, not unlike the new sensation the boyfriend in the book had begun to notice. And it definitely wasn’t normal.“Oh, it’s probably just a lymph node,” I told myself as I read each page with increasing interest, my growing paranoia kept barely in check.
I convinced myself to get a CT scan just in case I was being blindsided by another health misfortune. After all, chronic lymphocytic leukemia had come as a complete surprise and I had no way of knowing if Pandora’s Box was still open, letting all sorts of nasty things out.
It turns out there was a happy ending to the book. The boyfriend’s tumor was benign. And there was a reasonably happy ending for me, too: it was just a node. I was about to start my second course of Rituxan therapy and I expected it to take care of the problem.
But four rounds of Rituxan later, the ALN was still there, though it had hardly earned its name at that point. As time went on I got used to it. The pressure increased almost imperceptibly. When I started eight rounds of Rituxan in October 2005, I hoped that might take care of it. No such luck.
During the early part of this year, the ALN grew from a minor sensation to a slight bother. I would notice it when sleeping on my right side, and when sitting. When Marilyn and I drove to Columbus, Ohio to see Dr. John Byrd, it was there -- not especially troublesome but present nonetheless. I asked Byrd about it, and he stuck his hand into the flesh next to my left hip and said, matter-of-factly and without any concern, “Yes, you have some deep pelvic lymph nodes.”
I asked Byrd whethe
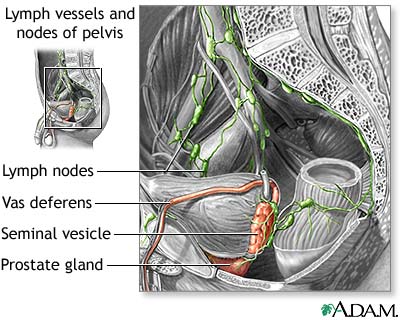 r I needed CT scans to monitor those and other nodes, and he said it wasn’t necessary. If, for example, a node were pressing on a kidney and becoming a problem, it would show up in the creatinine numbers on a chem panel.
r I needed CT scans to monitor those and other nodes, and he said it wasn’t necessary. If, for example, a node were pressing on a kidney and becoming a problem, it would show up in the creatinine numbers on a chem panel.My chem panels before and since have been marvels of normalcy. Whatever the ALN is pressing on, it apparently isn’t all that important. But it is noticeable, and during the last week or so it has entered the realm of chronic pain. Not horrible nerve-shooting-down-the-leg pain, which I have heard about in CLL. Just pressing and pressing and pressing, noticeable no matter where I sit, stand, or lay. I am not sure what water torture is like, but this could be similar. For the first time this past week I couldn’t sleep because of the pain and had to take an ibuprofen.
Now I realize that in the grand scheme of chronic pain this is nothing. It is not interfering with my life and daily business, just making things more uncomfortable. I rather enjoy ibuprofen and that will work for awhile, I suppose, but it is not a solution. Neither is asking my doctor for percocet or oxycontin. I can enjoy a few hours of spaciness as much as anyone, but it is not a way to live one’s life. I suppose there is acupuncture, or perhaps hypnosis, but these are, again, temporary solutions to a problem that will only get worse.
So the ALN has done what I have been expecting one of these days to happen: it is the symptom that heralds the end of watch and wait. The ALN is the other shoe that finally dropped. Nodes, abominable and otherwi
 se, appear to be my major symptom. My hemoglobin and platelets are still well within normal with no downward trend, meaning that marrow impaction is not an issue. (In fact, my latest CBC shows platelets going up.) I still have no B symptoms. Just a very thick neck (to match my thick skull) and a rather distended abdomen.
se, appear to be my major symptom. My hemoglobin and platelets are still well within normal with no downward trend, meaning that marrow impaction is not an issue. (In fact, my latest CBC shows platelets going up.) I still have no B symptoms. Just a very thick neck (to match my thick skull) and a rather distended abdomen.What is the aim of treatment? To reduce the nodes (and tamp the disease back down again). And to do this as part of my near-term treatment strategy. That strategy, simply put, is to use HuMax-CD20 when it arrives on the market, perhaps in 2008. My goal is to get from here to there, and then to use HuMax for as long as I can. Burn no bridges, play for time, the same old song, now with rhyme!
I meet with my local hem/onc later this month to formulate a treatment plan. What exactly that is yet, I don’t know. But it will involve Rituxan and very likely something else. The Abominable Lymph Node has got to go.





3 comments:
As I recall, you had treatment with rituximab as a single agent. Is that what you are considering for this bothersome node? I've read of your journeys...
The supposition, of course, is that HuMax will be approved. Nothing is written in stone, AYK. As the Paul Simon song goes (slip sliding away), 'God makes His plans; the information is not available to the mortal man.'
Have you thought about Chinese traditional medicine, honokiol, or something of that nature? I have a CLL friend who's been using honokiol, and she's been happy with the results.
As always, YMMV.
Very well written as always. I do not know if the groin nodes are the largest in the body but they have always been an issue for me as well although not to the extent you describe. Good luck.
Loren
Rituxan will be part of the treatment but I think I am past the point where it can be the only part of the treatment. I know Dr. Byrd thinks Rituxan 3 x week for 4 weeks may do better than the Rituxan schedules I have had in the past -- he is probably right -- but even then the prospect of 50% or greater node clearance lasting 10 months is only 40%. There may be an opportunity cost to my using that much Rituxan without adding something that is known to get those nodes down.
Candidates for addition to Rituxan are:
*a low-dose steroid such as dexamethasone, administered to reduce nodes prior to commencing Rituxan
*a high-dose steroid such as HDMP, a la UCSD
*chlorambucil
*GM-CSF
*Beta Glucan
Perhaps more than one of the above.
I am trying to nail down the logic and risks/rewards of some of these moves. I'll discuss that here when I get it settled.
I would be shocked if HuMax-CD20 doesn't make it to market. It has survived Phase 1/11, shows no unacceptable toxicity, and has FDA fast-track status. Plus from what I have heard, it really does seem to work better. It was developed in the lab of Dr. Martin Glennie, no slouch in the monoclonal biz. I would define it as a very realistic hope.
I have tried honokiol with no evident beneficial result. The same is true of EGCG. My case of CLL is more bulky and advanced than many; the really soft-glove stuff is unlikely to work. I do, of course, keep my eye out for such things. Beta Glucan as a Rituxan booster is one interesting idea.
Post a Comment